This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
The primary treatment goals for chronic obstructive pulmonary disorder (COPD) are centered around controlling symptoms, improving quality of life, reducing exacerbations, and reducing COPD-related mortality. 1 These goals represent unmet needs in current COPD management.2
Educational programs can help patients learn how to take their medication properly and use oxygen devices correctly. These programs can also teach special inhalation techniques and offer advice on preventing and coping with acute breathing difficulties. There are numerous nonpharmacologic interventions that can potentially reduce mortality rates among patients with COPD, including:1,3





Some people with COPD lose a lot of weight over time. Their muscles become weaker, and they become less fit. For these patients, combining high-calorie supplements with regular weight management practices can help improve respiratory muscle strength, handgrip strength, weight gain, exercise performance, and quality of life.4
Nutraceuticals are gaining popularity as a therapy for treating disease symptoms in patients with chronic diseases. Quercetin is a plant flavonoid with potent antioxidant, anti-inflammatory, anti-infectious, anti-hypertensive, and blood glucose-lowering properties. Daily oral treatment with low-dose quercetin reduces oxidative stress and inflammation, prevents lung disease progression, and inhibits rhinovirus-induced epithelial damage and replication, a primary trigger of COPD exacerbations.. A small, double-blind, placebo-controlled clinical trial was conducted to determine the efficacy of quercetin in reducing markers of oxidative stress and inflammation in the lung in patients with COPD. The study enrolled 14 patients with COPD between 40% and 70% predicted and randomized to placebo or quercetin 2000 mg/day in a 1:2 ratio. Patients taking quercetin, but not placebo, showed significantly reduced levels of IL-8, IL-1β, and 8-isoprostane in bronchoalveolar lavage (BAL) and surfactant protein-D (SP-D) in serum. C-reactive protein (CRP) levels did not change in either group.
Oral and inhaled medications are used for patients with stable COPD to reduce dyspnea, improve exercise tolerance, and prevent exacerbations. There are two main options for delivery of inhaled medications, by inhalers or nebulizer.6

Hydrofluoroalkane inhalers (HFAs) deliver medication in liquid form as an aerosol spray from a pressurized canister. These portable devices act quickly on the airways with one or two puffs administered over a few seconds. Proper use involves priming, shaking the inhaler before use, coordinating actuation with inhalation, inhaling slowly and steadily, and holding one’s breath. Using a spacer can enhance delivery of the full medication dose to the patient’s lungs.7
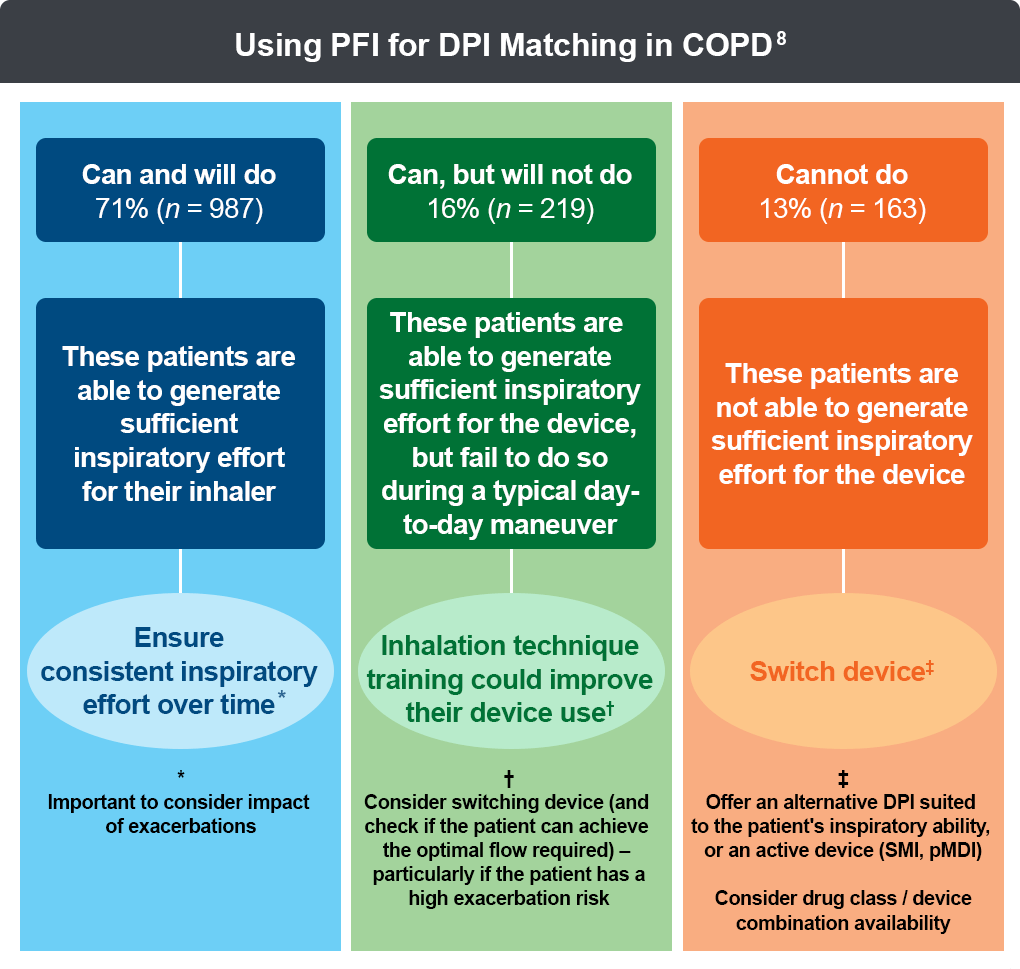
A dry-powder inhaler (DPI) is similar to HFA, but it releases a puff of dry powder instead of a liquid mist. DPI devices are breath-actuated, and the amount of medication reaching the lungs depends upon the aerosol characteristics. This is created by the patient’s inspiratory maneuver overcoming the internal resistance of the device and dispersing the dry powder medication, separating the drug from carrier particles.6 Therefore, for optimal DPI matching, it is recommended to measure a patient’s peak inspiratory flow (PIF), in addition to observing inhaler technique.8
A soft mist inhaler (SMI) is a more advanced type of inhaler that provides a measured amount of medicine in a slow-moving mist that helps the patient inhale the medicine. SMIs are portable devices that do not contain propellants and can be used in patients with lower inspiratory flow rates. SMIs also require hand–breath coordination and breath-holding.7
Nebulizers produce a fine mist of medication, for administration up to 20 minutes, and have been used for many years in COPD treatment. Nebulizers do not require priming, hand–breath coordination, or breath-holding, and aerosolize medication that the patient can inhale with regular tidal breathing. There are different types of nebulizers (jet, ultrasonic, and mesh), and each varies in speed of treatment administration, ease of operation, and portability. If a nebulizer is chosen, air-driven is preferred over oxygen-driven to avoid the potential risk of increasing partial pressure of carbon dioxide in the blood (PaCO2).9
Numerous studies have shown that incorrect inhalation device technique can compromise medication delivery, increase the risk of exacerbations, result in higher healthcare resource utilization, and lead to premature mortality.10,11
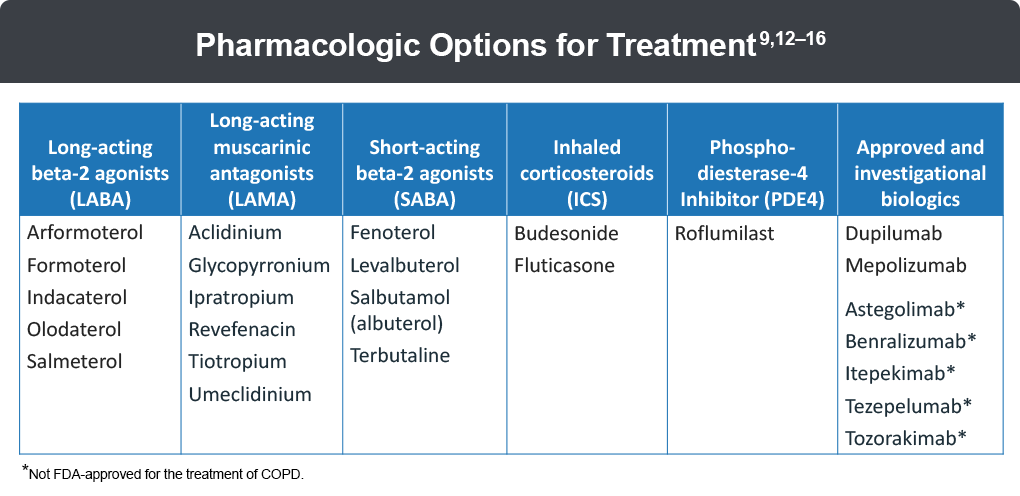
The recent phase 3 IMPACT and ETHOS clinical trials found mortality benefits with inhaled corticosteroid/long-acting muscarinic receptor antagonist/long-acting β2 agonist (ICS/LAMA/LABA) triple therapy compared with LAMA/LABA dual therapy in patient populations with symptomatic COPD at high-risk for future exacerbations.16
Despite current pharmacologic strategies with first- and second-line approaches, many patients with COPD remain symptomatic, with persistent symptoms and/or acute exacerbations as well as progressive loss of lung function, highlighting unmet needs in COPD management. Type 2 inflammation is seen in 20%–40% of patients with COPD and is one of the hallmarks of underlying pathophysiology leading to disease progression. Several novel therapeutics target type 2 inflammation (IL-4, IL-5, and IL-13) and the epithelial alarmins (IL-33 and TSLP) that contribute to the clinical features of COPD, and may help provide a tailored approach to treatment.2
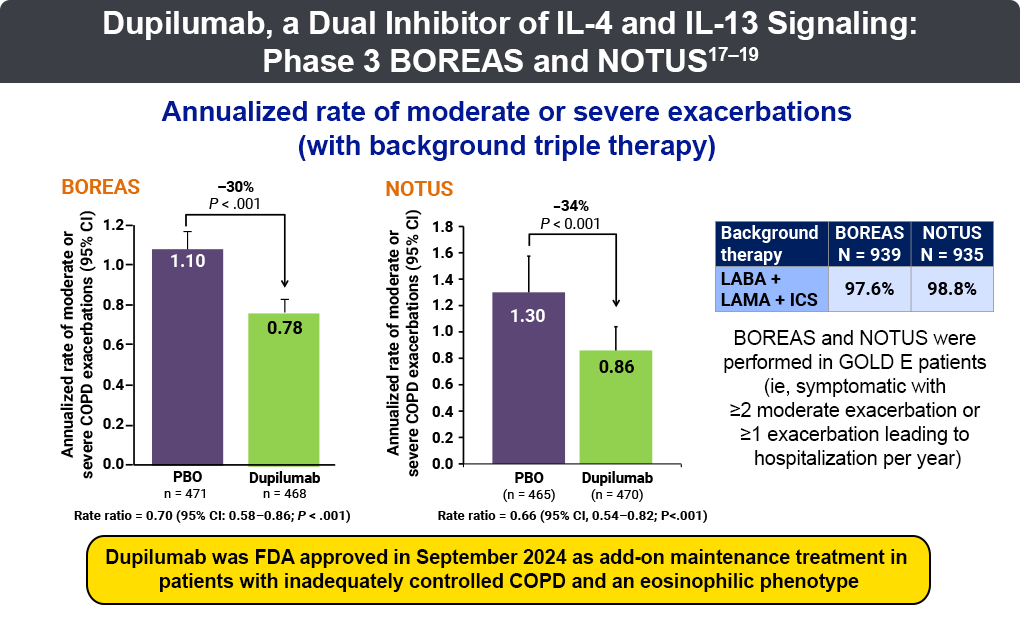
Dupilumab is the first US Food and Drug Administration (FDA)-approved biologic for add-on maintenance treatment of adults with uncontrolled COPD with an eosinophilic phenotype (blood EOS ≥300 cells/µL). Dupilumab is a mAb that inhibits the signaling action of IL-4 and IL-13 through binding of the IL-4R⍺ subunit of receptor complexes IL-4R⍺/𝝲C and IL-4R⍺/IL-13R.
The FDA approval of dupilumab was based on the BOREAS (N = 939) and NOTUS (N = 935) trials, which were double-blind, randomized, phase 3 trials of adults with blood eosinophil counts of ≥300/mL, with a primary endpoint of annualized rate of moderate-to-severe COPD exacerbations.17-19 Enrollment for both trials included adults who were current or former smokers aged 40 to 85 years and randomized to receive dupilumab or placebo added to maximal standard-of-care inhaled therapy.17-20 NOTUS confirmed the results from BOREAS; patients receiving dupilumab compared to placebo experienced:18,19
A pooled analysis of data from BOREAS and NOTUS found a similar proportion of patients reporting treatment-emergent adverse events (AEs) in both groups (72.1% dupilumab vs 71% placebo); AEs occurring in 5% or more of patients receiving either dupilumab or placebo included COVID-19 infection (6.9% vs 7.1%), upper respiratory tract infection (5.3% vs 6.1%), headache (7.8% vs 6.6%), COPD (5.3% vs 6.9%), nasopharyngitis (7.8% vs 7.4%) and accidental overdose (6.1% vs 6.6%). The proportion of patients with AEs leading to deaths were comparable (n = 19 for dupilumab vs n = 15 for placebo).21
Mepolizumab, the second FDA approved-biologic for add-on maintenance treatment in adult patients with uncontrolled COPD with an eosinophilic phenotype (≥150 cells/µL), is a mAb that inhibits IL-5 activity through direct cytokine binding.22,23
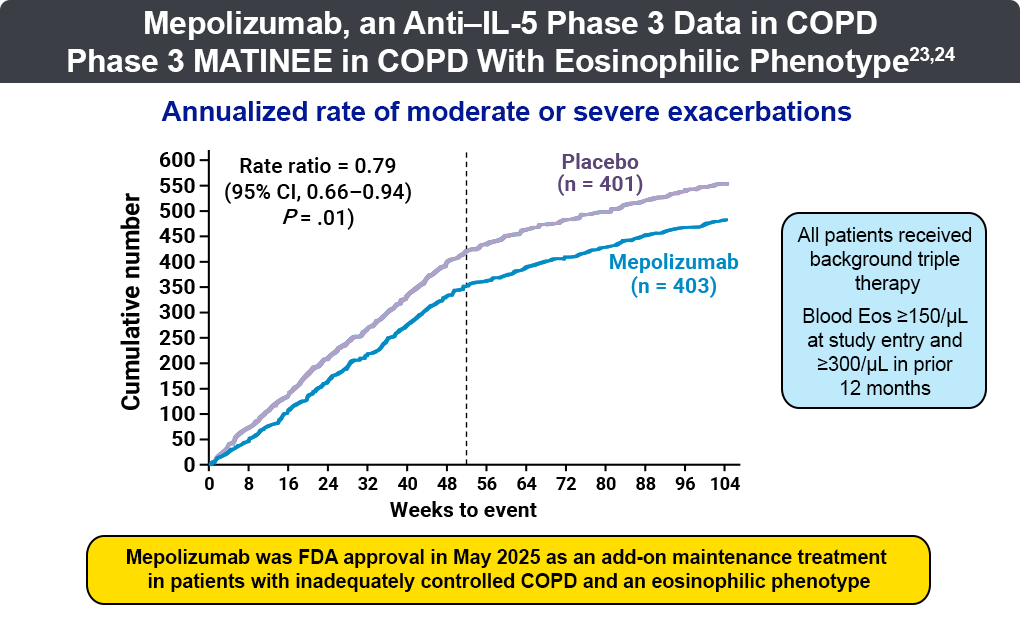
The FDA approval of mepolizumab was based on the MATINEE (N = 804) and METREX (N = 836) trials, which were phase 3, double-blind, randomized trials that assessed the efficacy and safety of mepolizumab 100 mg as add-on therapy in patients with stages 2-4 on the GOLD severity scale and with type 2 inflammation characterized by ≥300 cells/µL blood eosinophilic count (MATINEE) or in patients with blood eosinophilic count of ≥150 cells/µL at study entry or ≥300 cells/µL within the past year (METREX).23,24 An additional study, METREO, with the same clinical schema as METREX was also performed with 300 mg mepolizumab. The MATINEE study reported a significantly lower annualized rate of moderate or severe exacerbations with mepolizumab than with placebo (0.80 vs. 1.01 events per year; rate ratio, 0.79; [95% CI, 0.66 to 0.94]; P = 0.01) along with a delayed time to first moderate or severe exacerbation with mepolizumab than with placebo (419 vs 321 days; hazard ratio, 0.77; [95% CI, 0.64 to 0.93]; P = 0.009). The incidence of AEs was similar in mepolizumab and placebo groups. A meta-analysis randomized 1510 patients from METREX and METREO, 1136 patients were included in the pre-specified meta-analysis. Mepolizumab 100 mg subcutaneous (SC) significantly reduced annual moderate/severe exacerbation rates versus placebo by 18% (rate ratio: 0.82 [95% CI, 0.71-0.95]; P = .006), delayed time to first moderate/severe exacerbation (hazard ratio: 0.80 [0.68-0.94]; P = .006), reduced exacerbations leading to emergency department visits/hospitalization, and improved patient health-related quality of life.24
Benralizumab is another mAb that targets IL-5 activity by inhibiting binding of the IL-5R⍺ subunit of receptor complexes on eosinophils and basophils. GALATHEA (Benralizumab Efficacy in Moderate to Very Severe Chronic Obstructive Pulmonary Disease with Exacerbation History; N = 1044) and TERRANOVA (Efficacy and Safety of Benralizumab in Moderate to Very Severe Chronic Obstructive Pulmonary Disease with Exacerbation History; N = 1392) were two phase 3, double-blind, randomized, placebo-controlled trials. The primary endpoint was the effect of benralizumab on COPD exacerbation rates. Patients aged 40–85 years were assigned into an eosinophilic (>220 cells/μL) or non-eosinophilic (<220 cells/μL) group.25
Results of the GALATHEA study showed no significant improvements in annual rate ratios for exacerbations at any treatment dose. The same trend was detected in the TERRANOVA study. No dose effect related to benralizumab efficacy was detected, and similar adverse events were observed across studies. A patient subtype, with baseline blood eosinophil count ≥220 cells/mm, ≥3 exacerbations in the prior year, and receiving triple therapy, were the best responders, with exacerbation reductions with benralizumab (0.70; [95% CI, 0.56-0.88]).25
Itepekimab is an mAb that inhibits alarmin IL-33 through direct binding, A double-blind, phase 2a trial compared itepekimab (n = 172) with placebo (n = 171) in patients with moderate-to-severe COPD despite standard therapy, at 83 study sites in ten countries.26 Patients aged 40–75 years who were current or former smokers, had been diagnosed with COPD for at least 1 year, and were on a stable regimen of triple-inhaled or double-inhaled background maintenance therapy were randomly assigned to receive itepekimab 300 mg or placebo, administered as two subcutaneous injections every 2 weeks for 24–52 weeks. Annualized rates of acute exacerbations of COPD were lower in the itepekimab group (1.30, [1.05–1.61]) vs placebo (1.61, [1.32–1.97]), with a relative risk of (0.81 [0.61–1·07]; P = .13).26 When the analysis was restricted to former smokers, treatment with itepekimab was associated with nominally significant reductions in acute exacerbations of COPD (RR .58, [95% CI, 0.39–0.85]; P = .0061) and FEV1 improvement (least squares mean difference .09 L [.02–.15], P = .0076) compared with placebo.26
Two phase 3 clinical studies (AERIFY-1 and AERIFY-2) are ongoing to confirm the efficacy and safety profile of itepekimab in former smokers with inadequately controlled COPD. AERIFY-1 met the primary endpoint of a statistically significant reduction in moderate or severe acute exacerbations compared to placebo of 27% at week 52, a clinically meaningful benefit; AERIFY-2 did not meet the same primary endpoint, although a benefit was seen earlier in the trial.27,28
Astegolimab is an mAb that inhibits IL-33 activity by binding to its receptor, ST2, on parenchymal and inflammatory cells.12 In the single-center, randomized, double-blind, placebo-controlled COPD-ST2OP trial (phase 2a, N = 81), participants with moderate to very severe COPD were randomly assigned (1:1) to astegolimab 490 mg SC or placebo every (q) 4 weeks over 44 weeks.29,30At 48 weeks, overall exacerbation rates between the astegolimab and placebo arms were not significantly different (2.18 vs 2.81; P = .19) or in prespecified groups with high (>170 cells/µL) or low (<170 cells/µL) eosinophil counts (0.83 [0.49-1.40] vs .0.69 [0.39-1.21]). While astegolimab was not found to significantly reduce exacerbation rates, the health status of participants did improve compared with placebo.30
Tozorakimab is a promising monoclonal antibody under investigation for the treatment of COPD. It targets IL-13. It is a broad-acting epithelial “alarmin” cytokine targeting IL-33. Early safety, pharmacokinetic, and biomarker studies support the clinical development of this monoclonal antibody.31 Phase 2 data from FRONTIER-4 suggests that tozorakimab may improve lung function and reduce COPD exacerbations, especially in patients with frequent exacerbation history.32
Tezepelumab is an mAb that targets thymic stromal lymphopoietin (TSLP) through direct binding, inhibiting TSLP binding with its receptor. In a phase 2, randomized, double-blind trial, tezepelumab was evaluated over 52 weeks using 3 dosing levels (70 mg, N = 138; 210 mg, N = 137; 280 mg, N = 137) compared to placebo.33 Researchers reported a significant diminution of annualized asthma exacerbation rates for tezepelumab over placebo (62% dosed at 70 mg q4 weeks, 71% dosed at 210 mg q4 weeks, and 66% dosed at 280 mg q2 weeks; P < .001).33 Pre-bronchodilator FEV1 was also slightly higher in all tezepelumab-treated groups, independent of baseline blood eosinophil counts.33 COURSE (Tezepelumab COPD Exacerbation Study), a phase 2a, multicenter, double-blind, randomized trial evaluated the efficacy of tezepelumab on moderate or severe COPD exacerbation rate ratios across 90 sites in 10 countries. The annualized rate of moderate or severe COPD exacerbations over 52 weeks was 1.75 for tezepelumab versus 2.11 for placebo (rate ratio 0.83 [90% CI, 0·64-1.06]; P = 0.10 [one-sided]; the primary endpoint was not met); however, prespecified subgroup analyses points to further study in patients with moderate-to-severe COPD and with a blood eosinophilic count of ≥150 cells/µL. AEs occurred in 133 (81%) of 165 patients in the tezepelumab group and 126 (75%) of 168 patients in the placebo group.34
All URLs accessed August 25, 2025
This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
