This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory disorder affecting the airways, lung parenchyma, and pulmonary vasculature.
This condition is characterized by persistent, poorly reversible airflow limitation, and prominent respiratory symptoms, including chronic cough, dyspnea, and sputum production. The pathogenesis of COPD is driven by increased oxidative stress and an imbalance between proteases and antiproteases. Notably, cigarette smoke induces oxidative stress (Figure), activating macrophages and epithelial cells to release chemotactic factors that recruit neutrophils and CD8+ T-cells from the circulation to the lungs.
The severity of inflammation generally correlates with the degree of airflow obstruction. Inflammatory cells release mediators that stimulate fibroblasts, leading to aberrant repair processes and bronchiolar fibrosis. Additionally, an imbalance between proteases (released by neutrophils and macrophages) and antiproteases results in alveolar wall destruction (emphysema) and obstructive physiology. Proteases also contribute to mucus hypersecretion. Elevated oxidant burden, stemming from smoke inhalation or inflammatory leukocytes, prompts epithelial cells to release chemotactic factors, inactivates antiproteases, and directly damages alveolar walls, further promoting mucus secretion. Protease-mediated elastin degradation leads to loss of elastic recoil, resulting in airway collapse during exhalation.

The inflammatory response drives airway obstruction, reflected by a reduced forced expiratory volume (FEV1) and causes tissue destruction, further exacerbating airflow limitation and impairing gas exchange. This leads to gas-trapping and hyperinflation of the lungs, often visible on imaging studies. As the disease progresses, gas exchange impairment worsens, with reduced ventilation or increased physiologic dead space contributing to CO2 retention. Pulmonary hypertension may develop due to diffuse vasoconstriction secondary to hypoxemia.
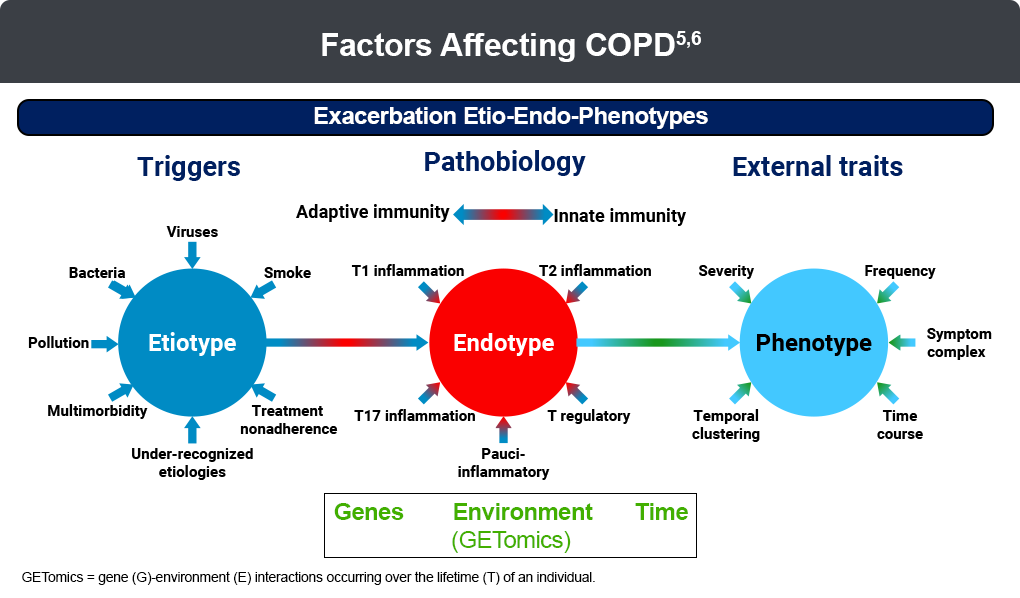
Acute exacerbations of COPD, commonly triggered by bacterial or viral infections or environmental irritants, are frequent and are associated with accelerated lung function decline and prolonged reductions in quality of life. Recent research has identified distinct etioendophenotypes of acute exacerbations, categorized by clinical presentation, etiology, natural history, frequency, severity, and biomarkers (Figure).
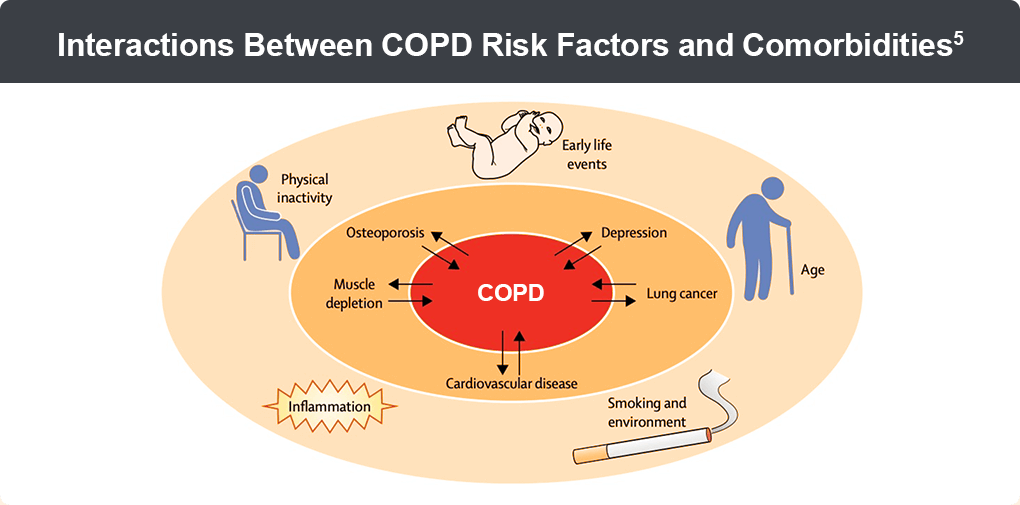
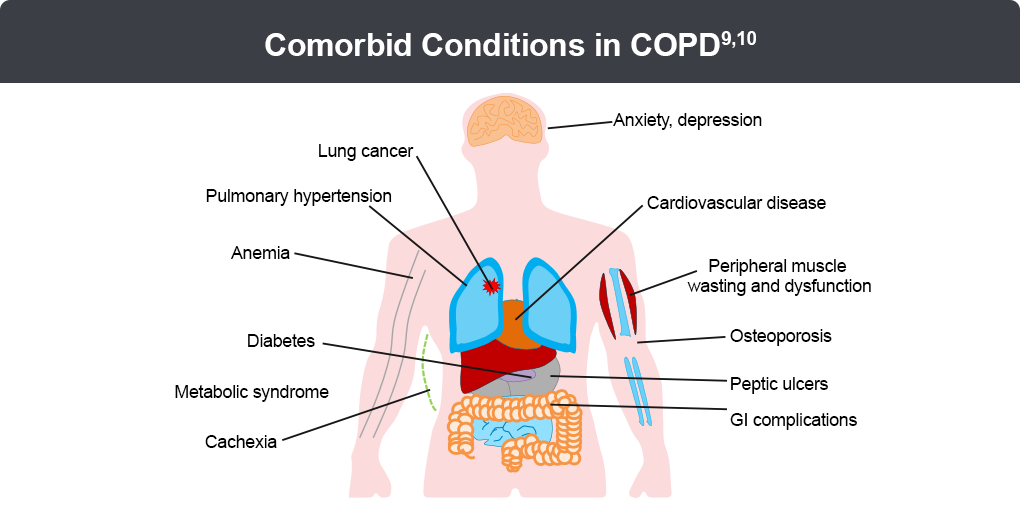
COPD often coexists with multiple comorbidities sharing common risk factors, such as advanced age, smoking, systemic inflammation, and physical inactivity, which may predispose individuals to COPD or exacerbate its course. Conversely, COPD may increase the risk of other chronic conditions through shared inflammatory and inactivity-related pathways (Figure). The interplay of comorbidities, such as pulmonary hypertension, cardiovascular disease, and lung cancer, significantly worsens COPD morbidity and mortality.7,8 Consequently, routine monitoring and management of comorbid conditions using a multidisciplinary approach are essential for optimizing patient outcomes.9-12
This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
